
9 Focused Assessment- Neurological Examination
Learning Objectives
At the end of this chapter, the learner will:
- Obtain the health history of the neurological system.
- Assess the neurological system of the patient including the cranial nerves, sensory function, pain, temperature, and position sense of a patient.
- Document findings of the neurological exam.
I. Overview of the Neurological System
The assessment of the neurological system includes examinations of mental status, level of consciousness, and neurological function. While details of the mental status assessment will be described in the next chapter, this chapter will begin with a review of the 12 pairs of cranial nerves and their functions. It will follow with a collection of important terminologies related to this system and then continue with key assessment components for the system.
II. Anatomy and Physiology
Click the link below to review the anatomy and physiology of the neurological system. In the assessment process, you will need to apply your knowledge of the 12 pairs of cranial nerves and their functions to the neurological system.
A more detailed review of neurological system is available at the link:
III. Medical Terminology
The following are commonly used medical terminologies in the assessment of neurological system.
| Affect | observable behaviors that indicate a person’s feelings or emotions |
| Anxiety | a feeling of uneasiness or discomfort experienced in varying degree |
| Apathy | lack of emotional expression; indifference to stimuli or surroundings |
| Aphasia | a neurological condition in which language function is absent or impaired |
| Cognitive functioning | an intellectual process by which one becomes aware of, perceives, or comprehends ideas |
| Coherency | conversation and behavior that conveys thoughts and feelings in a logical and relevant manner |
| Cerebrovascular Accident (CVA) | a stroke; a blockage or the rupture of a blood vessel in the brain |
| Delirium | a temporary state of confusion |
| Depression | a mood disorder characterized by low mood, a feeling of sadness, and a general loss of interest in things |
| Dementia | impairment of intellectual functioning, memory, and judgment |
| Dysarthria | speech disorder involving difficulty with articulating and pronunciation of specific sounds |
| Dysphagia |
difficulty in swallowing |
| Dysphasia | difficulty with speech |
| Encephalitis | inflammation of the brain |
| Hyperesthesia | abnormally increased sensitivity to sensory stimuli such as touch or pain |
| Labile emotions | unpredictable, rapid shifting of expression of feelings |
| Paralysis | loss of muscle function and or sensation secondary to nervous impairment |
| Paraplegia | a form of paralysis that affects in the lower half of the body |
| Paresis | impaired muscle strength or weakness |
| Paresthesia | abnormal sensation such as numbness, tingling, or burning |
| Quadriplegia | a form of paralysis that affects all four extremities |
| Transient Ischemic Attack (TIA) | A neurological event with the signs and symptoms of a stroke, but which go away within a short period of time |
| Temporomandibular joint (TMJ) | the hinge joint between the temporal bone and the lower jaw |
Terms to Classify Altered Level of Consciousness
| Consciousness | normal |
| Confusion | disoriented; impaired thinking and difficulty following commands |
| Delirium | a temporary state of confusion; restlessness, hallucination, sometimes delusions |
| Lethargy/Somnolence | a state of severe drowsiness can be aroused by moderate stimuli |
| Obtundation | decreased alertness, slowed psychomotor responses; similar to lethargy |
| Stupor | responds only to intense and repeated stimuli; almost unconscious |
| Coma | a profound or deep state of unconsciousness; may lack a gag reflex or a pupillary response |
*Use Glasgow Coma Scale (GCS) to objectively assess the extent of impaired consciousness. The GCS is described later in this chapter.
IV. Step by Step Assessment
- Perform hand hygiene.
- Check room for contact precautions.
- Introduce yourself to patient.
- Confirm patient ID using two patient identifiers (e.g., name and date of birth).
- Explain process to patient.
- Assemble equipment prior to starting exam.
- Be organized and systematic in your assessment.
- Use appropriate listening and questioning skills.
- Listen and attend to patient cues.
- Ensure patient’s privacy and dignity.
- Apply principles of asepsis and safety.
- Check vital signs.
| Steps | Additional Information |
|
Ask relevant questions related to a past or recent history of head injury, neurological illness or symptoms, confusion, headache, vertigo, seizures, recent injury or fall, weakness, numbness, tingling, difficulty swallowing (dysphagia) or speaking (dysphasia), and lack of coordination of body movements. |
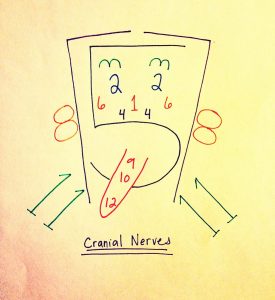
| 3. Assess the functions of the 12 cranial nerves. See chart below for more details.
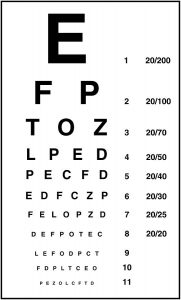
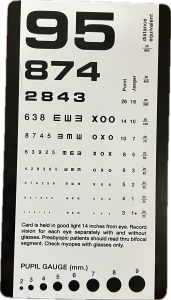
CNI – Assess smell CNII- Assess visual acuity using Snellen chart. CNIII/IV/VI – Assess extraocular eye movements using the 6 cardinal directions of gaze. Ask the patient to keep their head still and move only eyes. Instruct the patient to follow the examiner’s finger or an object as it moves in 6 directions: up, down, left, right, and diagnollay in both upper and lower directions.
CN V – Assess jaw clench by aking the patient to clench their teeth while the examiner palpate the masseter muscles for strength. Evaluate sharp and dull sensation over three branches of the trigeminal nerve (forehead, cheek, and chin) bilaterally. Use a cotton swab or a similar tool to apply sharp and dull stimuli, ensuring to compare sensations on both sides. CN VII – Ask the patient to raise eyebrows, smile, puff out cheeks, show teeth, and squeeze eyes shut. Observe for symmetry and strenght in these facial movements. CN VIII – Assess hearing by either whispering a word or number close to the patient’s ear or by lightly rubbing the examiner’s fingers next to the ear. Ask the patient to repeat what they hear or indicate when they hear the sound. CN IX /CN X – Assess swallowing by asking the patient to swallow. Observe for any difficulty or discomfort. Check the movement of soft palate by asking the patient to say “ah” and watching for symmetrical elevation of the soft palate. Evaluate the gag reflex by gently stimulating the back of the throat with a tongue depressor and noting the presence or absence of the gag response. CN XI – Assess the motor function of the spinal accessory nerve by asking the patient to shrug their shoulders while the examiner applies downward pressure. The trapezius muscles should be strong and symmetric. Note any weakness or asymmetry in shoulder elevation. CN XII – Assess tongue movement by asking the patient to stick out their tongue and move it from side to side. The tongue should be midline and not deviating to either side. |
CNII- Normal vision is 20/20. The top number represents the distance at which the patient can see the letters, while the bottom number indicates what a person with normal vision can see at that same distance.
CNIII/IV/VI – Assess extraocular eye movements using the 6 cardinal directions of gaze. 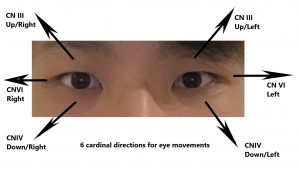
  |
4. Assess motor strength and sensation.
|
Unequal motor strength and unusual sensation may indicate underlying neurological disease or injury, such as stroke or head injury.
   Expected findings should be equal strength bilaterally, no pain, numbness, and or tingling sensation. |
| 5. Report and document assessment findings and related health problems according to agency policy. | Accurate and timely documentation and reporting promote patient safety. |
Knowledge Check
Assess 12 Cranial Nerve Functions
Click all hyperlinks to access more details.
| Mnemonic | # | Name | Function (Sensory/Motor/Both) | Assessment |
| On | I | Olfactory | Smell (S) | |
| Old | II | Optic | Vision (S) | Visual acuity Visual field |
| Olympus’ | III | Oculomotor | Eye movements (M) |
Eye movements (CN III, IV, VI) |
| Towering | IV | Trochlear | Eye movements (M) | |
| Tops | V | Trigeminal | Sensory/motor – face (B) | Facial movement and sensation |
| A | VI | Abducens | Eye movements (M) | |
| Finn | VII | Facial | Motor – face, taste (B) | Facial motor function |
| And | VIII | Auditory (Vestibulocochlear) | Hearing/balance (S) | Hearing |
| German | IX | Glossopharyngeal | Motor – throat, taste (B) | Movement of the soft palate and gag reflex
(CNIX and X) |
| Viewed | X | Vagus | Motor/sensory – viscera (autonomic) (B) | |
| Some | XI | Spinal Accessory | Motor – head and neck (M) | Shrug shoulder |
| Hops | XII | Hypoglossal | Motor – lower throat (M) | Tongue |
Copyrighted materials used with permission of the author, A. Chandrasekhar, Loyola University Medical Education Network.
Table adapted from Biga et al. Anatomy & Physiology. https://open.oregonstate.education/aandp/chapter/13-3-spinal-and-cranial-nerves/
Watch the cranial nerve assessment video below. In this video, the examiner uses ophthalmoscope to check the fundus of the eye (optic disc), a procedure that bedside nurses typically do not perform during routine head-to-toe or shift assessments.
Knowledge Check
Glasgow Coma Scale (GCS) Assessment
Glasgow Coma Scale is used to assess the level of consciousness in patients with acute brain injury or trauma in emergency situations. It evaluates three components: eye, verbal, and motor responses. Eye response assesses the patient’s ability to open their eyes spontaneously or in response to stimuli; verbal response evaluates the patient’s ability to speak coherently or respond to questions; motor response measures the patient’s ability to move their limbs in response to commands or stimuli.
A fully awake and alert person scores the highest at 15, while a person in a deep coma or with minimal response receives the lowest score of 3.
| Response | Scale/Score |
|
Best eye-opening response Record “C” if eyes closed due to swelling. |
Spontaneously (4)
To speech (3) To pain (2) No response (1) |
| Best motor response (to painful stimuli)
Press at fingernail bed and record best upper-limb response. |
Obeys verbal command (6)
Localizes pain (5) Flexion – withdrawal (4) Flexion – abnormal (3) Extension – abnormal (2) No response (1) |
| Best verbal response
Record “E” if endotracheal tube is in place, and “T” if tracheostomy is in place. |
Oriented x 3 (to person, time, and place) (5)
Conversation – confused (4) Speech – inappropriate (3) Sounds – incomprehensible (2) No response (1) |
- Click the link to get a more detailed overview of the GCS: Glasgow Coma Scale
V. Documentation
A sample narrative documentation:
Alert and oriented (x4) to situation, person, place, and time. Behavior appropriate to situation and developmental age. Clear speech and follow verbal commands. Cranial nerves II to XII grossly intact. Pupils Equal, Round, React to Light and Accommodation (PERRLA). Active range of motion all extremities with symmetry strength. Peripheral sensation intact.
VI. Related Laboratory and Diagnostic Procedures/Findings
Depending on the patient’s signs and symptoms from the physical examination, various diagnostic tests may be performed. For example:
- Blood Tests: These include tests such as complete blood count (CBC), electrolytes, thyroid function tests, and specific markers for infections or autoimmune conditions. The purpose of these blood tests is to identify infections, inflammatory processes, or metabolic abnormalities that may affect neurological health.
- Cerebral Angiography: This test visualizes blood vessels in the brain by injecting a contrst dye into the blood vessels, helping to detect abnormalities like aneurysms, stenosis, or arteriovenous malformations.
- Electroencephalogram (EEG): This test measures the electrical activity in the brain and can be used to diagnose seizures, psychiatric disorders, and other brain conditions.
- Imaging Studies: Techniques such as Magnetic Resonance Imaging (MRI) or Computed Tomography (CT) scans are used to diagnose specific neurological disorders by providing detailed images of the brain and spinal cord.
- Lumbar Puncture (Spinal Tap): This test collects a sample of the patient’s spinal fluid to check for infections in the brain or spinal cord, or to identify potential brain cancer.
A more detailed overview of different neurological diagnostic tests is available at: Neurological Diagnostic Tests and Procedures
Evidence-based Practice

Pupillometry
Changes in pupillary size and reaction to light are early indicators of neurological changes. However, in critically ill patients, judging pupillary reactions—whether brisk, sluggish, or absent—can be challenging.
A pupillometer provides an objective and reliable measurement of pupillary size and reactivity. It offers accurate assessments that can detect changes in a patient’s condition early, allowing for proactive treatment and resulting in a better outcome (Romagnosi et al., 2022).
VII. Learning Exercise
VIII. Attributions and References
- Biga, L. M., Dawson, S., Harwell, A., Hopkins, R., Kaufmann, J., LeMaster, M., Matern, P., Morrison-Graham, K., Quick, D., & Runyeon, J. Anatomy & Physiology. http://library.open.oregonstate.edu/aandp/chapter/13-3-spinal-and-cranial-nerves/#tbl-ch13_03
- Chandrasekhar, A. (March 28, 2006 updated). Screening Physical Exam. http://www.meddean.luc.edu/lumen/MedEd/medicine/pulmonar/pd/contents.htm
- Doyle, G. R. & McCutcheon, J. A. Clinical Procedure for Safer Patient Care. https://opentextbc.ca/clinicalskills/chapter/2-5-focussed-respiratory-assessment/
- Hacking, C. & Gaillard, F. Radiopaedia.org. https://radiopaedia.org/articles/olfactory-nerve?lang=us. Accessed July 20, 2019.
- Michael Gibson, C., Bahekar, P., & Sharfaei, S. WikiDoc: Glasgow coma scale. https://www.wikidoc.org/index.php/Glasgow_coma_scale. Accessed July 20, 2019.
- National Institute of Neurological Disorders and Stroke. https://catalog.ninds.nih.gov/sites/default/files/publications/neurological-diagnostic-tests-procedures.pdf. Accessed August 7, 2024.
- Orlando, G. (2006). Animation that illustrates the pupillary light reflex. Public domain via Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Eye_dilate.gif
- Psychology Wiki https://psychology.wikia.org/wiki/Level_of_consciousness. Accessed 7/16/2021
- Romagnosi, F., Bernini, A., Bongiovanni, F., Iaquaniello, C. Miroz, J., Citerio, G., Taccone, F. S., & Oddo, M. (2022). Neurological pupil index for the early prediction of outcome in severe acute brain injury patients. Brain Sciences 12, 609. https:// doi.org/10.3390/brainsci12050609
