

1 Health Assessment and Clinical Judgment
Learning Objectives
After completion of this chapter, the learner will:
- relate the importance of health assessment to clinical judgment and quality of patient care
- discuss the types of health assessment
- differentiate objective from subjective data
- use techniques of physical assessment
- identify proper patient positions during physical examination
Overview of this Chapter:
This chapter will introduce the concept of clinical judgment, its significance to nursing practice, quality of care and how health assessment is an integral component of this concept. Sound clinical judgment requires nurses to be competent in several aspects of assessment such as recognition and interpretation of cues , which are prerequisites of taking actions to address the identified problems. This chapter will introduce overview of clinical judgment and health assessment, types of data, types of assessment, techniques of physical examination and positioning during physical examination.
Health Assessment and Clinical Judgment
Sound nursing clinical judgment is at the core of competent and safe client care ( Dickison et al, 2019). Clinical judgment is made up of actions and behaviors dependent on cognitive, psychomotor behaviors and affective processes. Accurate patient assessment is needed to provide appropriate intervention. Assessment includes recognizing relevant cues, not only from direct patient assessment but information from the environment, health history, laboratory values. This is an essential step of clinical judgment so that the nurse can proceed to analyze these cues, form hypothesis of the relationships of cues and prioritize problems to act on. Benner ( 2004) describes nursing practice as varied and complex and often undertermined, that good nursing practice requires that the nurse develop skillful ethical comportment and use of good clinical judgment informed by scientific evidence and technological development. Furthermore, Benner ( 2004) asserts that perceptual acuity in recognizing salient signs, symptoms and responses to therapies are required for the clinician to use good clinical judgment in particular cases. These illustrations of the necessity of clinical judgment support the need for the nurse be competent in health assessments, and that health assessment must be informed by sound clinical judgment as well.
The National Council of State Boards of Nursing (NCSBN) Clinical Judgment Measurement Model synthesizes three established and accepted paradigms for clinical judgment that are used in educating nurses ,as a framework in the creation of test items to test clinical judgment in licensure examinations ( Dickinson, et al 2019). The NCSBN-CJM is presented in the figure below:
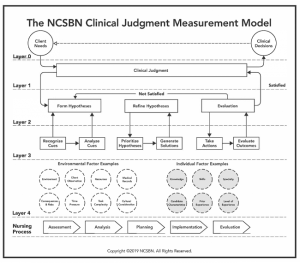
The nursing process includes five components of problem solving such as assessment, nursing diagnosis, planning, implementation and evaluation. It is a useful tool for beginning students as foundation for problem solving client problems, it does not encompass the complexities of clinical reasoning and the factors that influence it ( Tanner, 2006). The NCSBN’s six step clinical judgment model delineates the process for making clinical judgments such as ( Billings and Kowalski, 2019):
a. recognizing cues :
- identifying cues from the environment
- patient observations
- information from health records such as laboratory values, health history, prescriptions
- distinguishing relevant from irrelevant information
b. analyze cues:
- using knowledge to interpret cues and make inferences
- recognizing relationships among data points
c. prioritize hypotheses:
- listing possible client problems
- identifying priorities
d. generate solutions
- identifying possible solutions to the problem
- selecting solutions with evidence for best outcomes
e. take action
- implementing the solution
f. evaluate outcomes
- determining results of actions
- changes in vital signs
- effects of treatments and pharmacologic interventions
- compare actual outcomes with expected outcomes
The following are key points on clinical judgment:
- Nursing practice had increased in both complexity (acuity levels of clients, decreased length of hospital stays) and responsibility (career development, differences between novice and experienced nurses); nurses transitions through five levels of proficiency: novice, advanced beginner, competent, proficient, and expert (Benner, 1984; Dreyfus & Dreyfus, 1987). Benner incorporated these five stages of skill acquisition into her definition of nursing clinical judgment
- Tanner (2006), in developing the Model of Clinical Judgment, recognized intuitive-humanistic as one type of reasoning that nurses use in addition to analytic and narrative reasoning, acknowledging that nurses go back and forth among these types of reasoning. Tanner explained that less experienced nurses, including students, may rely more heavily on analytic reasoning, whereas experienced nurses are more likely to use intuitive reasoning based on their clinical experiences. Lasater’s (2007) research expanded Tanner’s aspects of clinical judgment, based on experienced nurses, to describe a trajectory of clinical judgment development for students. Tanner recognized that nurses’ backgrounds, both clinical and personal, impact what they notice about patients. An example of this is when an expert nurse accurately anticipates the needs of a client based on his or her previous experiences.
- Nurses require deep knowledge to make decisions that result in optimal client outcomes (Benner, Tanner, & Chesla, 2009). As nursing students move on the continuum from novice to greater expertise in practice, their ability to recognize and analyze cues, prioritize hypotheses, and generate solutions for clients, based in evidence and experiences with clients, increases. Their concrete experiences in clinical practice serve to guide their actions and improve their clinical judgment. Knowledge gained from formal education is layered with concrete experiences are important aspects of the nurse’s education.
- Importance of context (i.e., client and environmental factors, and characteristics of the nurse him- or herself) to a nurse’s clinical decision-making ability (Croskerry, 2009).
- Clinical judgment is an adaptive strategy that lies between analytic thinking and intuitive thinking, depending on the context; nursing actions that require decision making can be viewed on a continuum ranging from intuitive thought to analytical thought, based on the features of the action (complexity, ambiguity, and presentation) that influence the thinking processes of the nurse.
- The iterative processes in clinical judgment: recognize cues, generate hypotheses, judge hypotheses, take action, and evaluate outcomes; the back and forth process allows for identification of the process and identification of points of error. Clinicians must use prerequisite knowledge and skills to guide them when organizing information, and because of this, NCSBN focused on decision making situated within context-specific conditions. Clinicians must first recognize and analyze the cues associated with the clinical problem. Hypotheses are activated and generated based on the cue inputs. After hypotheses are prioritized, nurses will attempt to resolve the current problem by taking action based on the leading hypothesis.
The NCSBN Clinical Judgment Measurement Model will be used as the framework for the structure and activities of this open educational resource: ” Guide to Health Assessment for Nurses”.
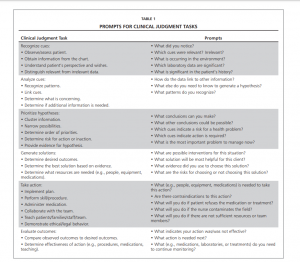
Systematic health assessments are performed regularly in nearly every health care setting. The nurse must be competent in performing health assessments for safe and quality patient care. Nursing health assessment is an incredibly valuable tool nurses have in their arsenal of competencies, where iterations of the key tasks of clinical judgment may happen. A thorough and skilled assessment allows the nurse, to obtain insights into the patient’s condition through cognitive and psychomotor processes to discover any associated physical findings and interpret cues that will aid in the decision to act accordingly. The decision to perform correct and ethical assessment techniques at opportune times are illustrations of good clinical judgment. Below are clinical judgments tasks and mental prompts for nurses:
Highlight: Illustrating Clinical Reasoning and Clinical Judgment
The following are basic information about health assessment:
Types of Health Assessment:
Health assessment is performed by nurses and other providers alike. The following are the types of health assessments performed by nurses in various situations. A health assessment is guided by the nurses knowledge of anatomy and physiology , therapeutic communication skills, pathophysiology, among others.
- Comprehensive head-to-toe assessments are done when a patient is admitted. This often times called a nursing admission assessment. A shorter comprehensive head to toe assessments are also performed at the beginning of each shift, and when it is determined to be necessary according to the patient’s hemodynamic status and context.
- Brief physical assessments are done as necessary and to identify changes in a patient’s status and for comparison with the previous assessment.
- Focused assessments are done in response to a specific problem recognized by the nurse as needing further assessment of a body system.
- Emergency assessments are done in emergency situations. Because of the emergent nature of many health conditions, the nurse may modify the assessment to obtain necessary information to provide emergent care.
- A routine physical assessment reveals information to supplement a patient’s database. The assessment is documented according to agency policy, and unusual findings are reported to appropriate members of the health care team. Ongoing, objective, and comprehensive assessments promote continuity in health care.
In all the types of assessment previously mentioned, the nurse will always collect subjective and objective data, the extent of data collection will depend on the purpose and the clinical context of the health assessment.
The ability to think critically and interpret patient behaviors and physiologic changes is essential. The skills of physical assessment are powerful tools for detecting both subtle and obvious changes in a patient’s health. The nurse must develop competency in patient assessment in order to provide safe patient care. A more detailed discussion of the most common types of assessment performed will be discussed in the next chapters of this guide.
Types of Data: ( cues identification)
Subjective Data:
Information that is reported by the patient or a reliable historian who is knowledgeable about the patient’s health related information is organized in a report called health history. The health history is taken and updated with each patient encounter as necessary; such information informs patient care. A more detailed discussion of health history is found in Chapter 2 of this guide.
Objective Data:
Objective assessment data includes that which is observable and measurable (Jarvis, 2012). Objective data observation and measurement is done through a systematic physical assessment procedure using various assessment techniques, measurement of vital signs and correlation of physical manifestations with laboratory and diagnostic findings.
Observation- using the senses : auditory- heart sounds; feel= moisture; smell= wounds( odor);
Measurement- value of a construct related to an assessment technique, compared to normal values or condition such as pain using the pain scale with the normal value of 0= no pain; weight= o as non and measured by a weighing scale; tenderness etc….
Techniques of Physical Assessment
The standard method of physical examination resolves around the following techniques.
- Inspection, which is considering clues from what we see.
- Palpation, gathering information from what we feel or what the patient feels as we palpate.
- Percussion, listening to different percussion notes and interpreting these in the context of the presenting complaint.
- Auscultation, using a stethoscope to listen more intensely to sounds within the body.
All of these aspects of examination rely on a knowledge of what is normal in order to identify any abnormalities. Physical assessment also requires some knowledge of common patterns of presentation or manifestations associated with different conditions.
All of the information gathered during these four techniques will add to clues and help nurses formulate nursing diagnoses or patient’s functional health problems. When we inspect our patient to discover relevant clues we look at the patient as a whole. Are they appropriately dressed for the current weather? Their demeanor? their expression? Does their facial expression indicate that they are in pain? Their gait? their body shape? If we are focused on specific systems, we may inspect one or more parts of the body related to that system.
Our hands can tell us many things about the body of the patient we are examining. As we shake hands with the patient at the beginning of the consultation we are aware if the patient’s hand is hot, which may indicate a fever, or cold, possible peripheral vascular problems, whether it is clammy, sepsis or cardiogenic shock. We can assess their muscle tone, limb weakness, or spasticity through palpation. All within the few short seconds of a handshake and as we move into specific system examinations we can palpate for tactile fremitus, respiratory, masses, abdomen or skin, pulses, circulation, lymph nodes, systemic infection or crepitus, musculoskeletal system.
One of the most difficult techniques for nurses to learn has been shown to be percussion of the body cavities. Percussion can give us clues to several health conditions by the change in the percussion note or sound when we percuss over solid, bone, tumor, fetus, feces, or fat or liquid, pleural effusion, urinary bladder ascites, or gas. Flatus, fully expanded lung tissue etc. The technique is to use the middle or index and middle fingers of your dominant hand as the drumstick and drop it smartly onto the middle phalanx of your non-dominant middle finger which rests on the patient’s body. The drum beat noise that this produces indicates whether solid, liquid or gas is present in that body cavity. Here are some examples of the sounds you could hear. Solid, over bone, liquid, over ascites, gas, over chest cavity.
Auscultation is the act of listening to body parts and assessing the sounds made using a stethoscope. There are several types of stethoscope and it is important to acquire a stethoscope which is appropriate to yourself and suitable for your patient group. For example, if you have a hearing deficit, an electrically amplified stethoscope may be useful for you. If you work mainly with babies and children, you may need a pediatric stethoscope which has a smaller head. You need to accustom yourself to your chosen stethoscope ensuring that the ear pieces are inserted pointing towards your face and not towards the back of your head. This way, they follow the ear canal and transmit sound more efficiently.
Exercises: Match the following images using your knowledge of physical examination techniques:
How to Perform the Techniques of Physical Examination
The order of physical assessment techniques usually occur in the following order: inspection, palpation, percussion, and auscultation. Use them in sequence—unless you’re performing an abdominal assessment. Palpation and percussion can alter bowel sounds, so you’d inspect, auscultate, percuss, then palpate an abdomen.
- Inspection
Inspect each body system using vision, smell, and hearing to assess normal conditions and deviations. Assess for color, size, location, movement, texture, symmetry, odors, and sounds as you assess each body system.
2. Palpation
Palpation requires you to touch the patient with different parts of your hands, using varying degrees of pressure. Because your hands are your tools, keep your fingernails short and your hands warm. Wear gloves when palpating mucous membranes or areas in contact with body fluids. Palpate tender areas last.
Types of palpation:
Light palpation
- Use this technique to feel for surface abnormalities.
- Depress the skin ½ to ¾ inch (about 1 to 2 cm) with your finger pads, using the lightest touch possible.
- Assess for texture, tenderness, temperature, moisture, elasticity, pulsations, and masses.
Deep palpation


- Use this technique to feel internal organs and masses for size, shape, tenderness, symmetry, and mobility.
- Depress the skin 1½ to 2 inches (about 4 to 5 cm) with firm, deep pressure.
- Use one hand on top of the other to exert firmer pressure, if needed.
3. Percussion
Percussion involves tapping your fingers or hands quickly and sharply against parts of the patient’s body to help you locate organ borders, identify organ shape and position, and determine if an organ is solid or filled with fluid or gas.
Types of percussion:
Direct percussion
This technique reveals tenderness; it’s commonly used to assess an adult’s sinuses.
- Using one or two fingers, tap directly on the body part.
- Ask the patient to tell you which areas are painful, and watch his face for signs of discomfort.
Indirect percussion
This technique elicits sounds that give clues to the makeup of the underlying tissue. Here’s how to do it:

- Press the distal part of the middle finger of your nondominant hand firmly on the body part.
- Keep the rest of your hands off the body surface.
- Flex the wrist of your nondominant hand.
- Using the middle finger of your dominant hand, tap quickly and directly over the point where your other middle finger touches the patient’s skin.
- Listen to the sounds produced.
4. Auscultation
Auscultation involves listening for various lung, heart, and bowel sounds with a stethoscope.
- Provide a quiet environment.
- Make sure the area to be auscultated is exposed (a gown or bed linens can interfere with sounds.)
- Warm the stethoscope head in your hand.
- Close your eyes to help focus your attention.
How to auscultate
- Use the diaphragm to pick up high-pitched sounds, such as first (S1) and second (S2) heart sounds. Hold the diaphragm firmly against the patient’s skin, using enough pressure to leave a slight ring on the skin afterward.
- Use the bell to pick up low-pitched sounds, such as third (S3) and fourth (S4) heart sounds. Hold the bell lightly against the patient’s skin, just hard enough to form a seal. Holding the bell too firmly causes the skin to act as a diaphragm, obliterating low-pitched sounds.
- Listen to and try to identify the characteristics of one sound at a time.
Prepare a patient for physical examination
Click the link to watch a brief video. Observe how the nurse prepare the patient to have physical examination.
References:
Introduction to Patient Assessment: https://opentextbc.ca/clinicalskills/chapter/introduction-2/
Shinnick, M.A. and Cabrera-Mino, C. ( 2021). Predictors of nursing clinical judgment in simulation. Nursing Education Perspectives. Vol 42, No 2; pp 107-109.
Learning Clinical ( Free) 2006. Assessing patients effectively: Here’s how to do the basic four techniques
Nursing2006: November-December 2006 – Volume 8 – Issue 2 – p 6
